
The people who gather around the Connectivity Table each week represent various health and social service agencies. Some are executives; some are front-line workers. But when they come together, it’s to collaborate and pool expertise. And to take action.
The situations brought to the Table involve individuals and families facing elevated risk – in immediate need of support.
The people who gather around the Connectivity Table each week represent various health and social service agencies. Some are executives; some are front-line workers. But when they come together, it’s to collaborate and pool expertise. And to take action.
The situations brought to the Table involve individuals and families facing elevated risk – in immediate need of support.
Connectivity Waterloo Region, which has initiatives in Kitchener and Cambridge, Ont., tailors its solutions to the person or family in front of them. Every situation is unique and requires a unique mixture of social services.
The risk factors being weighed by Connectivity partners are complex and numerous – 26 categories have been identified. Often they are related to mental health, criminal involvement or substance abuse. Housing, suicide risks and physical health are also major players.
The Kitchener group has noted a striking number of situations involving young adults (under age 24), teens and children. Issues such as mental health, addiction, poverty, precarious housing and the negative effects of peers all can place young people in a situation of elevated risk.
Kelly Niall, a physician’s assistant working with K-W 4 Health Links, who has been a member of Connectivity for almost two years, says it is fascinating to see how the group’s different perspectives focus on the various problems. “It feels like meaningful work,” she notes.
Niall’s employer, K-W 4 Health Links, works with people who have “medically complex” situations. Other partners at the Connectivity Table draw from various aspects of community services, from police to hospital services and from education to housing support. The Kitchener-based Table has about 30 partners and Cambridge about 25.
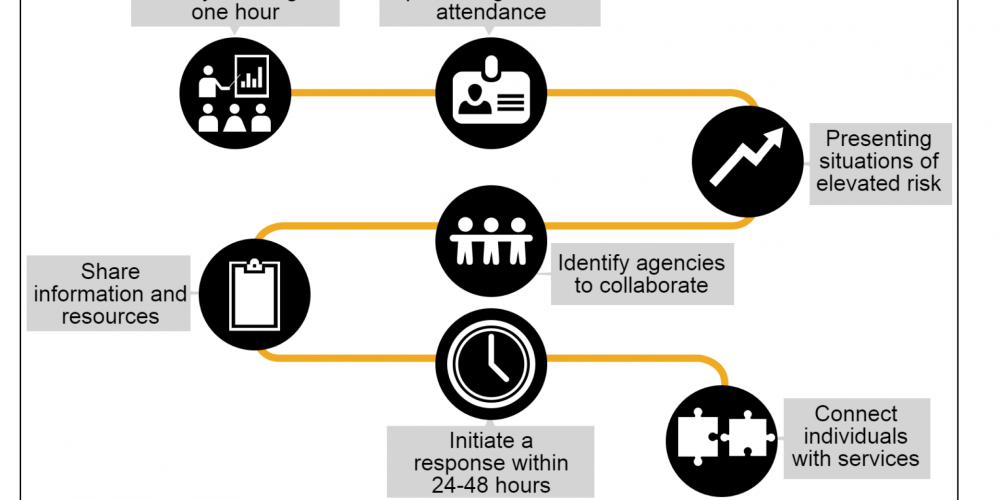
Roadmap of the Connectivity process
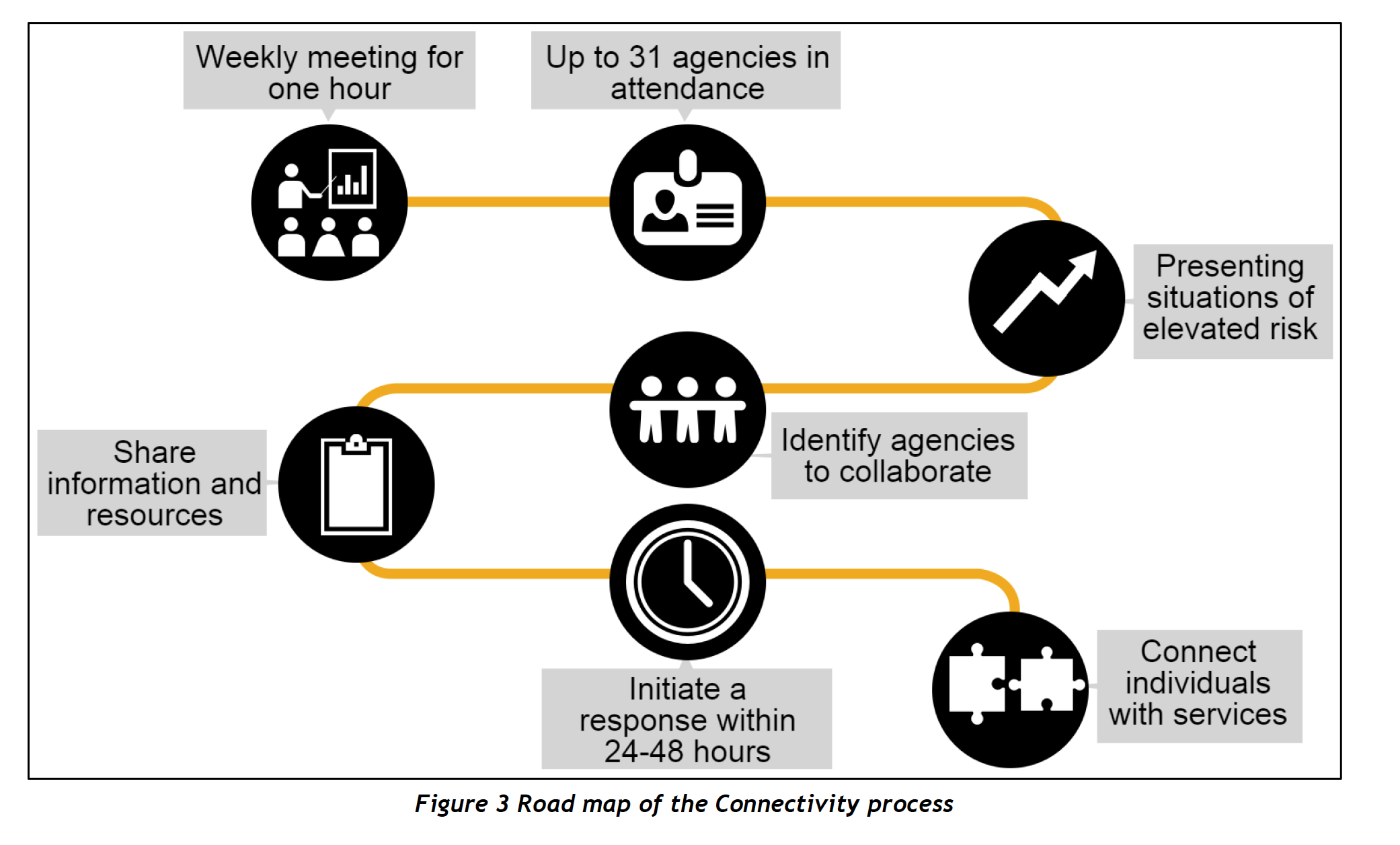
Confidentiality at the Connectivity Table is paramount. There are four filters that occur at various spots on this flow chart of the Connectivity process. This allows the partners at the table to screen situations without using personal information of the individual or family’s risk assessment.
Source: Carizon Family and Community Services.
The model for Connectivity comes from Prince Albert, Saskatchewan, where the Community Mobilization Hub has been taking a multidisciplinary approach to problem-solving since 2009. Prince Albert credits the initiative for a decline in violent crimes as well as decreases in child-protection caseloads, emergency room visits, mental health interventions and a variety of other social concerns.
After seeing the ingenuity and successes of the Saskatchewan program, the idea was brought to Waterloo Region through the Waterloo Wellington Local Health Integration Network, Waterloo Regional Police Service and the Waterloo Region Crime Prevention Council. The police and Langs created a Connectivity Table for Cambridge and North Dumfries in January 2014.
Later that year, a Kitchener Table was launched by Carizon Family and Community Services in partnership with the police. This initiative serves the cities of Kitchener and Waterloo plus Wilmot, Woolwich and Wellesley townships. It recently received a Smart & Caring Community Grant from the Kitchener and Waterloo Community Foundation.
Connectivity Waterloo Region has garnered international honours. In September 2015, it was a recipient of the IACP/Motorola Webber Seavey Award, given by the International Association of Chiefs of Police. The award honoured the Waterloo Regional Police Services’ collaboration with the community partners. It was presented at the IAPC conference in Chicago followed by a Kitchener celebration.
How Connectivity works
Any one of the member agencies can bring a situation to the Table, someone they’ve come across during their front-line work who is experiencing “acutely elevated risk.” The police bring about half of the cases to the Table.
Confidentiality is one of the highest principles of Connectivity. Situations are first presented without key identifying factors.
The Table partners then vote on whether the situation meets their threshold of “acutely elevated risk” to warrant immediate intervention. To fully understand this threshold, it is key to remember that many of the people accessing social services already live a life with varying levels of risk, some even quite severe, but for their case to come to Connectivity, something had to have happened that has elevated that risk. Connectivity is focused on that element and is designed to specifically address that factor.
Kitchener’s Connectivity Table
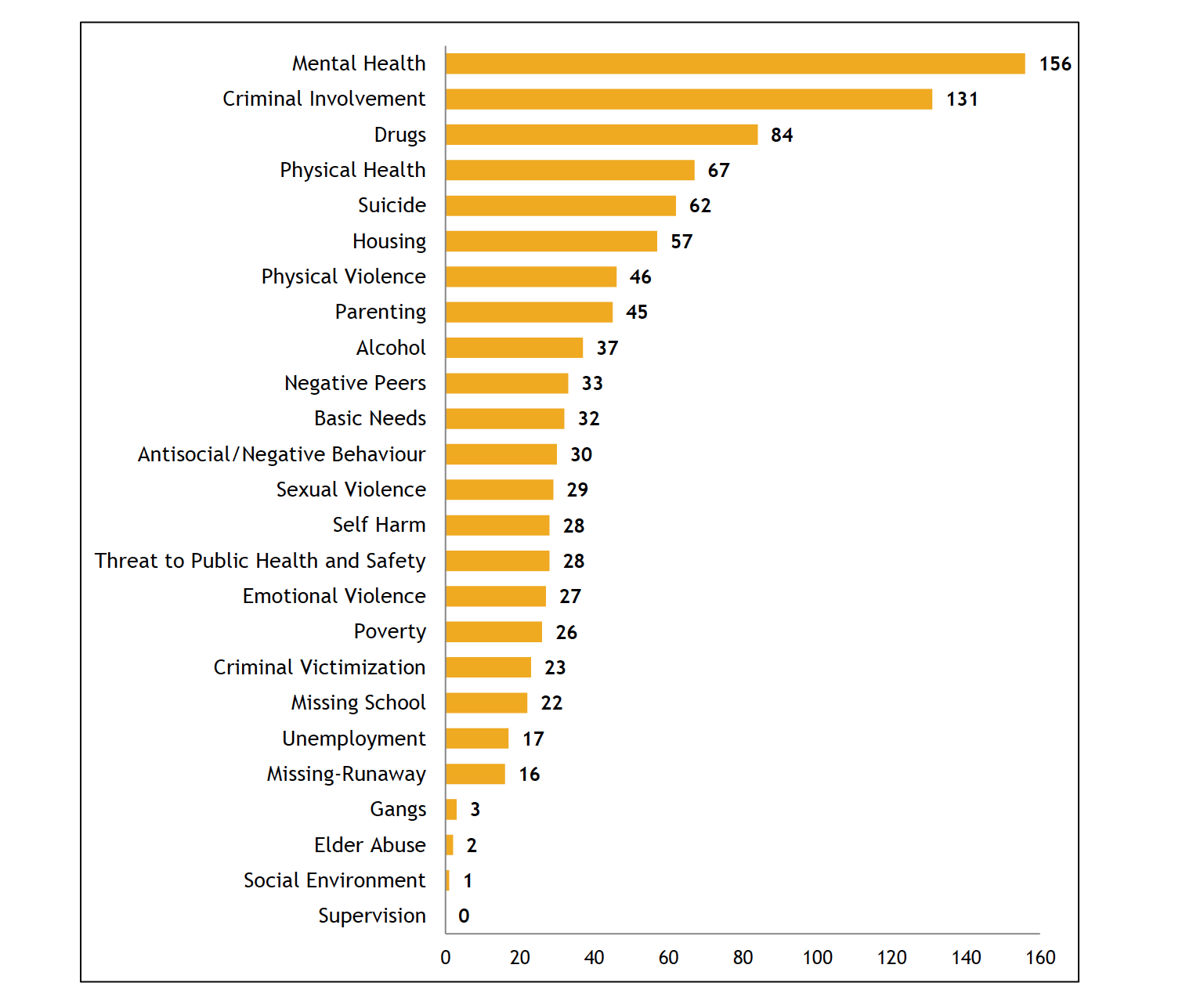
Each Connectivity Table accumulates data during every weekly meeting as each situation of an individual or family at an “acutely elevated risk” is assessed. The data fits into 26 defined categories, under which there are up to 102 risk factors. This data is a reflection of the category breakdown of the Kitchener Connectivity Table at its 18-month Report (October 2, 2014 to March 31, 2016).
Source: Carizon Family and Community Services.
If the case meets the threshold of elevated risk, further details about the individual are presented, such as name and address. Agency representatives with relevant information put up their hands, but give no details. Other agencies that might contribute to an intervention are identified. These agencies then meet away from the rest of the Table.
Next, all the organizations at the Table say whether they feel they can contribute to the case at hand. For any situation, four to six service organizations are usually involved.
These organizations then immediately meet, discuss the case, and develop a unique crisis plan to address the acute risk factor.
Obtaining consent is a priority that allows the process to move swiftly. Over 90 percent of people accept the help provided by the Connectivity Table.
Each table meets weekly and a key part of that is checking in with previously discussed cases. A week after a new situation is brought to them, the service organizations who volunteered to become involved give a report. If the crisis plan has been put into place and one of the organizations has taken the lead, the case is considered closed by the Table, though the work will continue, sometimes for years after the risk element has been mitigated.
Connectivity collects data in order to measure results, none of it identifiable. They keep track of the ages, genders and other statistical elements as well as the risk factors involved. This helps them track trends, notice patterns of violence and crime, as well as identify what new risk factors are emerging as the region changes, such as social isolation, which the Table and its member agencies have seen slowly increasing in their front-line work.
An 18-month report released in March 2016, showed 133 cases brought to the Kitchener Table. Of that, 121 were deemed “acutely elevated risk” and were opened as cases; 118 of those were fully concluded by the Table with three situations remaining still open. The 12 cases that were not seen were rejected because the individual was already connected to a service provider able to mitigate the risk.
Connectivity has seen a growth in the number of member and adjunct organizations involved as well as seeing more situations come before the Table. While an increase in cases could be seen as a negative statistic, instead it is positive one, indicating that more people are becoming aware of the initiative and, more importantly, more situations are able to be mitigated before an escalation occurs.
The Connectivity Table is an innovative and unique approach to policing, to social justice, and to delivering care. Its collaborative design instils a sense of community among its members, fostering relationships across all the social services.
Teghan Barton is a self-proclaimed Crackerjack Canadianist, having earned both an BA and MA in Canadian Studies where her focus is on issues of belonging, nationalism, and cultural policy. She is very passionate about social justice and working towards creating a safe and healthy future for the planet.